Most individuals with systemic lupus erythematosus (SLE) experience skin involvement or hair loss. There are many different types and, subsequently, various treatments. This article explores the relationship between lupus, hair, and skin.
NOTE: Johns Hopkins University Press, publisher of The Lupus Encyclopedia, is a nonprofit publisher. If you purchase JHUP books, like The Lupus Encyclopedia, you support projects like Project MUSE.
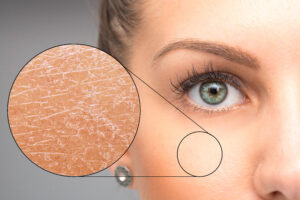
Lupus often presents many skin-related issues, ranging from rashes only seen in lupus to rashes that can be seen in other diseases. Cutaneous lupus erythematosus (CLE) refers to when lupus affects the skin. “Cutaneous” is the medical term for “skin.”
Discoid lupus is a common form of cutaneous lupus, marked by oval-shaped, scaly lesions., It can occur independently or as part of systemic lupus erythematosus (SLE). For example, someone can have discoid lupus by itself. Over time, around 20% of people with discoid lupus will have other organs affected by lupus. The person at this point is considered to have SLE. The cutaneous lupus (discoid lupus, in this case) is one of the complications of the person’s SLE, and the discoid lupus is the initial manifestation of SLE. Most people with SLE also have cutaneous lupus as part of their disease.
Nevertheless, other skin involvement can occur in lupus patients that are not exclusive to lupus and may be observed in other conditions. Examples of the latter include things such as livedo reticularis, vasculitis, telangiectasia, and erythema nodosum, to name a few. Chapter 8 of “The Lupus Encyclopedia” discusses the wide variety of cutaneous lupus lesions.
Hair Loss and Skin Problems: Unraveling the Connection
Reversible alopecia is due to SLE inflammation. The hair grows back when doctors successfully treat SLE by reversing inflammation around the hair follicles. However, if the inflammation permanently destroys the hair follicles, scarring alopecia occurs. Scarring alopeciameans the hair loss is irreversible and does not grow back. This primarily occurs when the hair loss is due to discoid lupus affecting the scalp. It is critical to seek urgent treatment with medications to manage SLE inflammation and prevent worsening. These treatments cannot reverse the damage and hairloss that has already occurred, but it can prevent its spread.
Understanding the emotional toll of hair loss is crucial. Hair loss is devastating for men and women with lupus and needs to be taken seriously.
Managing Challenges: A Holistic Approach
Addressing hair and skin problems in lupus necessitates a holistic strategy. Dermatological interventions may be employed, such as topical corticosteroids for skin issues or minoxidil for hair loss.
If you have hair loss, do not use the supplement biotin. There is no medical evidence that it works. Plus, it interferes with the results of numerous blood tests, including some autoantibodies and thyroid function tests.
Ask your doctor for minoxidil. Just 2.5 mg daily can help. You can also buy minoxidil solution over the counter to apply to the scalp twice daily. Note that positive effects can take as long as 6-12 months. Equally important is the broader management of lupus through medications that calm the overactive immune system.
Photosensitivity, an increased skin sensitivity to ultraviolet light (especially sunlight), is another common problem for all lupus patients. Although only 30% of SLE patients get a rash with sun exposure, all SLE patients’ lupus can get worse with UV exposure.
Ultraviolet (UV) light exposure can worsen skin involvement and trigger systemic lupus flares. Given the photosensitivity associated with lupus, robust sun protection becomes paramount. Patients should use broad-spectrum sunscreen, wear protective clothing, and avoid peak sunlight hours. Avoiding other UV light sources, such as using LED bulbs (instead of fluorescent or incandescent bulbs) in the home, is also essential. Unlike fluorescent and incandescent bulbs, LED bulbs emit much lower amounts of UV light. Therefore, avoiding UV light effectively is crucial to managing lupus. Click the UV light protection icon at the bottom of the “Lupus Secrets” page to learn more about good UV light protection habits.
Rlt: No, I do not have SLE. I do have alopecia, but I’m a 63 year old man where it runs in my family. My experience comes from caring for a large number of SLE patients for over 35 years plus close attention to the medical literature and all new research I can get my hands on.
Your feeling of your symptoms being so strange, not be similar to others, and nerve problems are not at all surprising. Every SLE patient is different. Some have never had any symptoms whatsoever, and their SLE was discovered on blood work. This person can even have life threatening SLE, such as severe thrombocytopenia or lupus nephritis (LN typically doesn’t cause symptoms until severe damage is already occurring.) Then on the other spectrum are patients with such severe symptoms that their quality of life is miserable. Since SLE can affect every organ of the body, do so from mild to severe, plus cause numerous different lab results: If I lined up 100 of my patients, none would be similar to each other.
In your case, if I had a patient like you, I’d need the help of a very good neurologist who has a special interest in complex cases. I’d want to know “where are the lesions?”, are they due to SLE or something unrelated? And if due to SLE is it due to permanent damage (for which all we could do is use nerve pain medicines) or due to potentially reversible lupus inflammation (for which we can use medicines like IVIG, rituximab, steroids, etc).
I hope you get the help you need, and thanks for sharing your story.




Leave a comment