People who have lupus have an increased risk for getting some cancers. Knowing what they are and how to prevent them is important, I discuss this in this blog post.
NOTE: Johns Hopkins University Press, publisher of The Lupus Encyclopedia, is a nonprofit publisher. If you purchase JHUP books, like The Lupus Encyclopedia, you support projects like Project MUSE.
UPDATE AUG 2024
Some experts question whether drugs like methotrexate cause basal cell cancer and squamous cell cancer. There are studies suggesting an increased association with these skin cancers in patients taking methotrexate and other immunosuppressants. However, some experts point out that these studies do not prove causality. A research flaw called “selection bias” may possibly contribute to incorrect results.
“Is lupus a type of cancer?”
This is not an uncommon question when someone is first diagnosed with systemic lupus erythematosus (SLE). Most newly diagnosed SLE patients have never even heard of lupus before. They want to know if it is contagious (the answer is “no”) and “is lupus a type of cancer?” Fortunately, the answer is “no.”
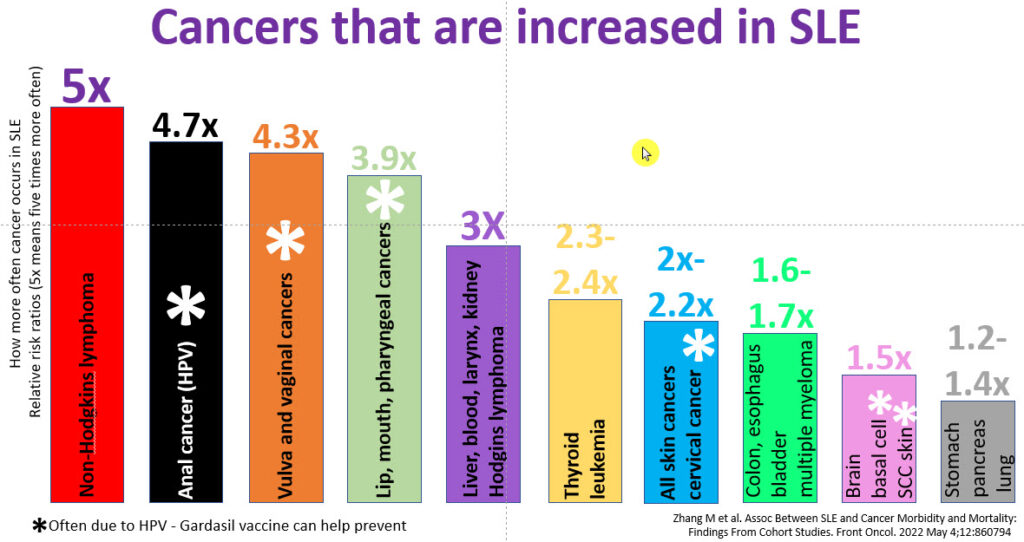
However, unfortunately, SLE patients are at increased risk of getting 24 types of cancer. This article will tell you which ones occur most commonly, but more importantly, it will tell you how to reduce your risk of getting many of them.
Lupus and Cancer: SLE patients get 24 cancers more commonly than the general population
Lupus Patients get Cancer More often than the General Population
A 2018 study by Song et al. reported 16 cancers occurring more commonly in SLE patients. This resulted in a flurry of online articles about lupus an cancer, discussing the article and its troublesome implications.
SLE is due to the immune system not working correctly. The white blood cells are responsible for removing cancer cells from our bodies as they occur. This occurs less efficiently in SLE patients.
SLE is a disease where the white blood cells are overactive and stay alive longer than they should. This could allow cancerous white blood cells to overtake the immune system (resulting in lymphoma, leukemia, or multiple myeloma)
SLE patients who smoke were especially at high risk, almost 2 ½ times more likely to die from lung cancer than non-lupus patients (Zhang et al). Smoking and lupus are a deadly combination for many reasons. I tell patients that stopping smoking is a requirement and doing so is non-negotiable.
It is crucial to catch cancers at an early, curable stage (do screening tests) and do things to prevent cancers… as listed below.
Reduce your Risk of Getting Cancer
This is the most important part of this blog post! There is good news! You can actively do things to reduce your risk of cancer significantly.
Get the Gardasil vaccine at 9 to 26 years old. The sooner, the better, hopefully before sexual activity. Note that of the first seven cancers occurring more commonly in SLE patients, six are due to HPV.
If you have a family history of breast cancer, and you have decreased bone density (osteopenia or osteoporosis), ask your doctor about raloxifene (Evista) to prevent breast cancer. Do NOT take raloxifene if you have antiphospholipid antibodies (ask your doctor); it can increase the risk of blood clots in people who are at increased risk.
Keep up with your cancer screening tests:
Important cancer screening tests for SLE patients include the following. Ask your doctor.
PAP smears
pelvic exams
mammograms
colonoscopies
chest CT scan (if there is a history of smoking)
prostate screening tests
thyroid exams
dermatologic skin cancer screenings (especially if you have sun-damaged skin or have been treated with cyclophosphamide, methotrexate, tacrolimus, or cyclosporin).
Yearly urine cytology in patients treated with cyclophosphamide (to rule out bladder cancer).
SLE patients tend to not keep up with these tests. We keep you so busy doing so many things; it is no wonder. However, it pays off to keep up with these. Ask your doctor.
I hope this information empowers the reader to work on preventing cancer and keep up with cancer screening tests to catch cancer early if it does occur.
For more in-depth information on cancer and lupus in greater detail:
It’s interesting to me that in 2000 I was diagnosed with aggressive BCell non Hodgkin’s lymphoma. It wasn’t until 2017 that I was diagnosed with Sjogrens and Lupus. My rheumatologist tested me for Sjogrens because, while she was taking my medical history on my first visit, I mentioned the history of NHL. She later explained the connection between Sjogrens and NHL. She suspected I had Sjogrens in 2000 but no one would have tested me for it then. I had consistently complained of dry eyes, throat, nose and ears, but again no one listened to me. Thankfully aggressive chemo put me in remission.
Are there blood tests that can be done to determine whether a patient has had/been exposed to EBV at any time in the past? Or can blood tests only detect an active case of EBV, not a past case of EBV?
Anon: Yes. IgG EBV is positive if you have had an EBV infection in the distant past. Many people were infected but did not get the full-blown mononucleosis infection (severe fatigue, fever, swollen glands, etc)
Donald Thomas, MD
This is important information to have – thank you very much for this detailed post!
Would it be possible someday to find or make a chart/graphic showing the absolute risk for each of these cancers for the general population compared to the lupus study population? This would be a very nice add-in to help put the relative risk into perspective.
I was relieved to see breast cancer isn’t on your list. I don’t have a history of breast cancer in my family, but I am taking Synthroid (which I read can increase chance of cancer?). I understand there is a higher rate of hypothyroidism in populations with Lupus than in the general population. Do you know if Lupus has any impact on that risk? Thank you for this great post!
you are correct about hypothyroidism from Hashimoto’s disease being more common in SLE patients. I do not think it impacts cancer risks (the SLE does)… however, I am not sure it has even been studied (so not sure). Some studies showed less breast cancer in SLE patients. However, that was always questioned because a high percentage of the patients in those studies were of racial backgrounds that also have lower risks. The more recent Zhang study showed similar rates of breast cancer in SLE as in the general public. Donald Thomas, MD
Jan Lee: Thank you for reading my post. The article from Taiwan, Wu CC et al suggested a 50% increase in some cancers in levothyroxine users. However, this is a great example of a study which can have major flaws. It is a retrospective study (goes backwards in time) rather than a prospective (forwards) randomized placebo-controlled trial (RCT, the best type). It does not remove other possibilities. For example, what is people with Hashimoto’s thyroiditis or people who have hypothyroidism automatically have an increased risk for cancers? We know this occurs in other autoimmune diseases (like lupus, Sjogren’s and rheumatoid). What we need is a prospective RCT of people with very mild hypothyroidism. Have half take Synthroid, the other half none… follow them over time, then see if there is a difference.
Great information to keep us vigilant In monitoring our health. With so many camera on the list, it will be nice when they have a blood test that screens generally for cancer-I thought I read that one is in development.
Dr Thomas thank you so much for keeping us informed so we can discuss matters with our health care providers. Is it possible to have Scleroderma even if it is not shown on a blood test? I have SLE and have been diagnosed Scleroderma of the esophagus after an endoscopy by a GI doctor. My rheumatologist tested me for Scleroderma and the blood test was negative. With Scleroderma of the esophagus is it possible that it will become systemic?
Thanks for writing this article very informative. If a patient is 45 years + they need to get the Gardasil vaccine? The article didn’t mention a higher age group.
Towanda: Great question. The answer is “yes.” Nothing is set in stone. If someone were 50 years old, out again on the dating scene, then it could be a good decision to get it. This is where the patient-doctor conversation comes into play regarding the pros and cons. I know I would probably want to get it. However, the cost would probably have to be covered by the patient. Insurance would most likely not cover it.
Great post! Question on the list of cancer screenings, do you have a list of what age to start those screenings or with what frequency? Is it the same standard screening frequencies as healthy people? Or is it a different schedule?
Dear Brandy: Thank you for reading my post and your kind words. I decided not to be specific regarding specifics on screenings. Reason being: the recommendations are repeatedly tweaked by the major cancer organizations as new science pops up (regarding age, who, when, how to deal with results, etc). Therefore, I left that part out and ask that people proactively discuss with their doctors.
Thank you very much Dr. Thomas for all your wonderful help. I’m wondering if you have an article on free kappa light chains in lupus, Mine were slightly high but the ratio was normal. I’m hoping to find information on this and how it relates to my SLE. My Rheumatologist ran this blood test. Also I’ve had tendon involvement in my hands/ fingers thumbs but normal sed rate. I’m wondering if there is an article or info on having this type of tendon involvement with normal sed rate. Thank you for your help.



Leave a comment